



![]()
![]()
![]()
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://nmj.umsha.ac.ir/article-1-2142-en.html


2- Professor, Mother & Child Care Research Center, Department of Medical-Surgical Nursing, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran
3- Professor, Department of Statistics, Faculty of Health, Hamadan University of Medical Sciences, Hamadan, Iran
4- Faculty Member, Research Center for Chronic Disease Care, Department of Medical Surgical Nursing, Faculty of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran ,
Medicinal nonadherence prevents the achievement of therapeutic goals in cardiovascular patients. Training is essential to increase medicinal adherence. Therefore, the present study compared the effect of two teach-back and pictorial training methods on the medication adherence in heart failure patients.
This quasi-experimental study was performed on 210 heart failure patients in Hamadan Heart Hospital in 2019. Patients were selected by convenience sampling and randomly assigned to one of three groups of Teach-back, pictorial, and control training. Training sessions were held in three sessions on three consecutive days. Data were collected using demographic and medication adherence questionnaire (MMAS-8) before, immediately and 6 weeks after training. ANOVA, ANCOVA and Repeated measures ANOVA statistical tests were used.he present study is a descriptive-cross-sectional study of the type of correlation. Third and fourth year undergraduate nursing students (due to more attendance at bedtime) and postgraduate nursing students at Hamadan School of Nursing and Midwifery in the first semester of the academic year were 2017-2018 were considered to be the research community (123 people). Sample students were selected from the students who had the criteria to enter the study and wanted to participate in the study, as a sample of the census. In order to collect data, a three-part questionnaire including demographic questionnaire, standard questionnaire of nurses' moral sensitivity in decision making and spiritual health questionnaire was completed by the sample individuals.
The Demographic Questionnaire consists of 5 questions related to individual characteristics (including age, sex, marital status, level of education and history of participation in the ethics workshop). The standard questionnaire for nurses' ethical sensitivity in decision making was developed by Nordin, Lützén and Brolin in Sweden [25]. Then, this questionnaire was used in different countries, including Iran. The validity of this questionnaire in Iran was assessed by Hassanpoor et al., whose reliability was 0.81 [15]. Pearson correlation coefficients were analyzed. It is worth mentioning that the level of significance in this study was considered to be 0.05.
There was no statistically significant difference between the three groups in medicinal adherence at baseline. Immediately after training, medication adherence was significantly higher in teach-back and pictorial groups than the control group (P<0.001), but there was no difference between teach back group and the pictorial group (P=0.123). Six weeks after training, medicinal adherence was significantly higher in teach-back group compared to the control and pictorial group (P<0.001). There was no significant difference between the two methods at different levels of education (P>0.05).
| Variables |
Study groups | P | ||
| Teach-Back (n=70) SD±M | Pictorial (n=70) SD±M | Control (n=70) SD±M |
||
| Age (years) | 8.52 ± 58.87 | 58.11 ± 62.14 | 13.06 ± 58.80 | 134/ a 0 |
| BMI (kg / m2) | 3.65± 26.45 | 4.67± 27 | 3.52± 26.30 | a0.547 |
| Systolic blood pressure (mmHg) | 18.32± 129.31 | 17.68 ± 136.91 | 17.68±133.50 | a0.056 |
| Diastolic blood pressure (mmHg) | 18.32 ± 25 /80 | 17.68 ± 81.58 | 12.62 ± 80.15 | a0.723 |
| Number of hospitalization days | 1.68 ± 7.17 | 1.73 ± 6.95 | 1.84 ± 7.10 | a 0.270 |
| N (%) | N (%) | N (%) | ||
| Gender Male Female |
(62.90) 44 (37.10) 26 |
(40.61) 43 (38.60) 27 |
(52.9) 37 (47.10) 33 |
b0.429 |
| Education Illiterate Primary Guidance High-school Diploma and above |
(8.60) 6 (60) 42 (10) 7 (12.90) 9 (8.60) 6 |
(10) 7 (65.70) 46 (12.90) 9 (7.10) 5 (4.30) 3 |
(7.10) 5 (37.10) 26 (22.90) 16 (17.10) 12 (15.70) 11 |
b0.020 |
| Marital status Single Married |
(2.90) 2 (97.10) 68 |
(11.40) 8 (88.60) 62 |
(11.40) 8 (88.60) 62 |
b 0.112 |
| Job status Has a job No job |
(64.30) 45 (35.70) 25 |
(65.70) 46 (34.30) 24 |
(61.40) 43 (38.60) 27 |
b 0.886 |
| Smoking Does Does not |
(25.70) 18 (74.30) 52 |
(30.24) 17 (75.70) 53 |
(28.60) 20 (71.40) 50 |
b 0.842 |
| Drug use Does Does not |
(11.40) 8 (88.60) 62 |
(14.30) 10 (85.70) 60 |
(15.70) 11 (84.30) 59 |
b 0.756 |
Table 2. Comparison of mean drug adherence of patients in three groups: pictorial, control and teach-back-oriented
| Groups | Upon arrival SD±M |
Right after training SD±M |
Six weeks after training SD±M |
Analysis of variance with repeated measures in each group | Analysis of variance with repeated measures between three groups |
| Teach-Back | 5.34± 11.37 | 4.62± 9.04 | 3.84± 6.12 | 182.49= F 2= df P>0.001 |
30.01= F 2= df * P>0.001 |
| Pictorial | 2.97± 11.04 | 3.10± 8.40 | 2.46± 9.31 | 23.736= F 2= df P>0.001 |
|
| Control | 4.13± 11.31 | 4.25± 10.85 | 3.94± 10.98 | 0.65= F 2= df P=0.519 |
|
| One-way analysis of variance and covariance | 0.119= F 2= df P=0.888 |
15.77= F 2= df * P>0.001 |
37.75= F 2= df *P>0.001 |
Table 3. Comparison of the average drug adherence of patients in the studied groups based on education (score from zero to 32)
| Education | Groups | N (%) | Upon arrival SD±M |
Right after training SD±M |
Six weeks after training SD±M |
Frequently measured variance test statistics |
| Illiterate |
Teach-Back | (8.6) 6 | 2.19± 12 | 2± 9.50 | 1.50± 6.83 | F=3.21 df=2 P=0.030 |
| Pictorial | (10) 7 | 2.03± 11.42 | 1.85± 7.71 | 1.39± 8.14 | ||
| Control | (7.1) 5 | 2.40± 12.60 | 2.19± 10.40 | 1.64± 13 | ||
| Primary |
Teach-Back | (60) 42 | 0.59± 11.11 | 0.58± 8.83 | 0.49± 5.59 | F=15.30 df=2 P>0.001 |
| Pictorial | (65.7) 46 | 0.56± 11.47 | 0.55± 8.91 | 0.47± 9.30 | ||
| Control | (37.1) 26 | 0.75± 12.42 | 0.75± 12.50 | 0.63± 12.30 | ||
| Guidance |
Teach-Back | (10) 7 | 1.63± 11.85 | 1.58± 9 | 1.37± 6 | F=3.54 df=2 P=0.016 |
| Pictorial | (12.9) 9 | 1.43± 10.33 | 1.40± 7.88 | 1.21± 9.44 | ||
| Control | (22.9) 16 | 1.07± 11.37 | 1.05± 11.06 | 0.90± 10.62 | ||
| Secondary |
Teach-Back | (12.9) 9 | 1.54± 12 | 1.34± 9.66 | 1.30± 7.11 | F=5.48 df=2 P=0.002 |
| Pictorial | (7.1) 5 | 2.07± 9.40 | 1.79± 6.40 | 1.75± 10.20 | ||
| Control | (17.1) 12 | 1.33± 10.33 | 1.16± 9.25 | 1.13± 10.25 | ||
| Diploma | Teach-Back | (8.6) 6 | 2.17± 11 | 1.88± 9.16 | 1.58± 5.33 | F=6.96 df=2 P=0.001 |
| Pictorial | (4.3) 3 | 3.07± 8.33 | 2.66± 7 | 2.24± 10.33 | ||
| Control | (15.7) 11 | 1.60± 9.09 | 1.39± 8.63 | 1.17± 8.27 |
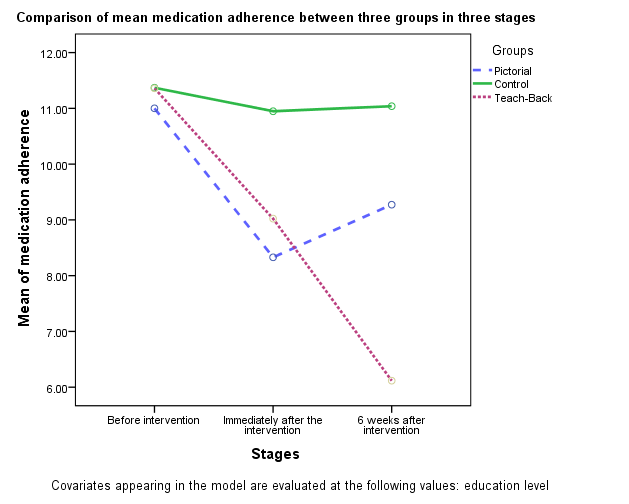
Figure 1. Comparison of patients' mean drug adherence in three groups of control, pictorial and teach-back-oriented
According to the results, teach-back training and pictorial methods have both improved patients' drug adherence immediately after training and six weeks after training compared to the beginning of the study. In the teach-back oriented group, there was a promotion of drug adherence at each stage compared to the previous stage, but in the pictorial education group, although drug adherence increased in the six weeks after training compared to the beginning, it was not significantly different compared to immediately after training. In the control group, which received only routine training, there was no change in drug adherence immediately after training or six weeks after training.
Consistent with the results of the present study, in the review study of Dinh et al. (2016) the effectiveness of teach-back method on self-care behaviors and its maintenance in health education of patients with chronic diseases was investigated; the results showed an improvement in adherence to the drug regimen in patients in the intervention group (23).
According to the results of the present study, immediately after training, drug adherence was significantly higher in the teach-back focused and pictorial groups than the control group, but there was no difference between the teach-back focused and pictorial groups. Six weeks after training, drug adherence was significantly higher in the teach-back oriented group compared with the pictorial and control groups. In other words, the maintenance and persistence of drug adherence in the teach-back oriented group was significantly higher than the pictorial education and control group. However, in the study of Negarandeh et al. (2013), both teach-back-oriented and pictorial training methods improved drug adherence in patients with diabetes and there was no significant difference between the two methods in the six weeks after training (24).
The results of the present study showed that in people with different levels of education, teach-back-oriented and pictorial education has led to the improvement of drug adherence immediately after training and six weeks after training, but there is a statistically significant difference in terms of teach-back-oriented and pictorial training on increasing drug adherence at different levels.
Teach-back training helps maintain medicinal adherence in heart failure patients. Therefore, it is recommended that nurses use this training method to improve medicinal adherence in these patients.
This research has been approved by the Research Ethics Committee with the ID IR.UMSHA.REC.1397.403. The researchers thank the Vice Chancellor for Research of Hamadan University of Medical Sciences for financial support and all the officials and nurses of the wards of Farshchian Heart Hospital in Hamadan who helped us in this research.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Received: 2020/02/4 | Accepted: 2020/04/13 | Published: 2020/05/30
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +9881 38380150
Publisher Tel: +988138381795
Website: http://nmj.umsha.ac.ir
Email: managingeditornmj gmail.com
gmail.com
