



![]()
![]()
![]()
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://nmj.umsha.ac.ir/article-1-1869-en.html

 , Leila Shirbeygi2 , Leila Farahani3 , Zainab Eslami Hasan Abadi4 , Morteza Shamsizadeh *5
, Leila Shirbeygi2 , Leila Farahani3 , Zainab Eslami Hasan Abadi4 , Morteza Shamsizadeh *5
2- Assistant Professor of Traditional Medicine, School of Persian Medicine, Department of Persian Medicine, Tehran University of Medical Sciences, Tehran, Iran
3- Department of Medical Surgical Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
4- Student Research Committee, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
5- Department of Medical Surgical Nursing, School of Nursing and Midwifery, Hamadan University of Medical Sciences, Hamadan, Iran
✅ The results showed that olive Oil and sweet almond massage is effective in preventing pressure ulcer. A similar study to this study should be done using other herbal products such as Aloe Vera gel to prevent Pressure ulcer.
Pressure ulcer is a complication from which many patients suffer causing eventually tissue necrosis. This type of ulcer is caused by the compression of the soft tissue of the body between a prominent part of the bone and a long outer surface [1].
The most common sites of pressure ulcer in the body are the back, sacrum, scapula, hip, iliac spine, heel and toe [12]. The pressure ulcers are severely divided into four degrees. These lesions range from reddish areas without altered skin, tissue destruction and necrosis to muscle and bone damage [14, 13].
The impact of pressure ulcers, in addition to reducing the level of health and complications in the patient, can also lead to heavy hospital costs and waste of time for nurses and medical personnel [18]. Prevention of this complication is a priority and a vital necessity in nurses' acute and long-term care plans; although it may happen despite all the efforts [19]. To this end, preventive measures can significantly reduce the cost of medical care [21,20]; and, by implementing some common and non-pharmacological measures, help maintain overall integrity of the skin [22].
One of the measures that nurses can take to protect skin and prevent pressure sores is massage. Nowadays massage is one of the therapeutic methods in the world that is dedicated to many clinical studies [25-23]. Massage using topical ointments is one of the ways to prevent acne in traditional medicine. The main mechanism of action of these oils is to hydrate the skin. Sweet almond oil, wheat bran oil and olive oil have these properties.
This study was a randomized clinical trial with three groups (control group and two experimental groups). The sample and the study population consisted of all patients admitted to ICU ward of Imam Jafar Sadegh Hospital in Meybod city with no pressure ulcer. Inclusion criteria included patients in ICU ward without pressure ulcers, inability to move or move with the aid of motor assisted devices only; exclusion criteria included any sensitivity after using olive oil or sweet almond oil, unwillingness to continue co-operation by the patient or his / her companions.
The sample size was estimated to be 98 people. Data were collected using a questionnaire, demographic and disease characteristics, and a checklist of prone wound sites for compression ulcers using Braden criteria. The sampling method in this study was initially available, then the samples were randomly selected and hexagonal blocks method was used. Six permutations were divided into three groups: letter A for control group, letter B for test group 1 (olive oil massage), and letter C for test group 2 (massage with sweet almond oil). Sampling was done until the number of samples was completed. After introducing themselves to patients or their companions the researcher explained the purpose of the study, then the eligible patients, who agreed to participate in the study signed the written informed consent. Considering gender differences, the research fellow was used to provide care and intervention to eligible patients. Participants in both experimental groups (massage with olive oil and sweet almond oil) were treated daily with olive or sweet almond oil in addition to routine treatment (changing position every 2 hours and wetting). Prior to massage, areas of pressure ulcer susceptibility were evaluated and the degree of pressure ulcer was determined if there was a pressure ulcer. Then the prone areas were massaged. The massage method was to first applying 1-3 mL of olive oil (in the test group 1) and sweet almond oil (in the test group 2) to the areas of the auricle, scapula, vertebral column, lumbar, gluteus maximus, iliac, and sacrum, elbows, heels and ankles (pressure areas) for gently massage. This daily intervention was performed in both groups for one week, and daily massage sites were monitored for the incidence of pressure ulcers. It should be noted that the olive oil needed for the study was purchased from Exir (Iran) and Sweet Almond Oil from Barij Essence (Iran). The data were analyzed with SPSS 16 (SPSS Inc., Chicago, Ill., USA). Depending on the type of data, descriptive and analytical statistics such as two-dimensional frequency distribution tables, three-group homogeneity tests, Chi-square test, Fisher exact test, and variance analysis were used to reach the goals.
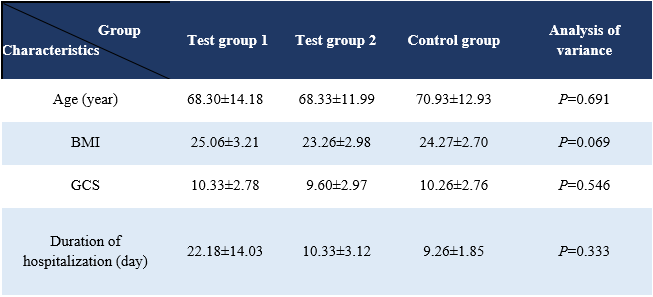
Table 1. Mean and standard deviation of age, BMI, GCS and hospital stay (days) by groups
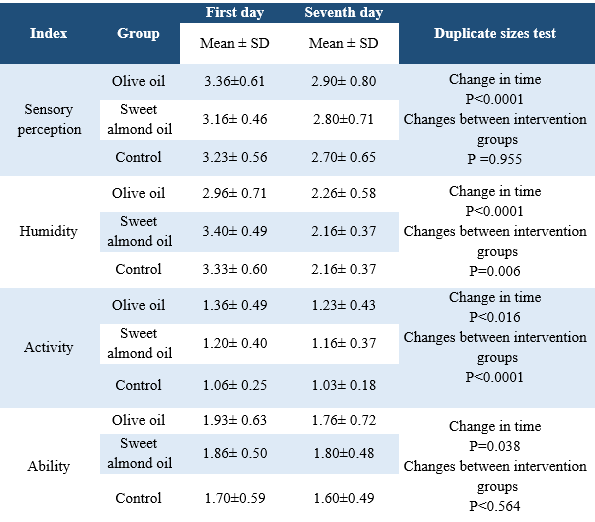
Results showed that mean and standard deviation of sensory perception and ability index in 7 days were significantly decreased (P<0.001). These changes were similar in all three groups and there was no significant difference between the three groups over time and overall (P>0.05).
The humidity variable decreased significantly over time (P<0.001) but the three groups did not decrease equally and according to the follow-up test, the least squares of the olive oil group decreased less rapidly than the control group (P<0.05). The mean and standard deviation of activity and nutrition variables decreased significantly over time (P<0.05). All three groups had significant differences. According to post hoc and pairwise comparisons, all three groups had significant differences (P<0.001).
The friction variable did not change significantly over time and there was no significant difference between groups (P>0.05). The sum of the indices of this instrument showed that there was a significant decrease over time between the groups. In fact, the groups had a statistically significant difference in terms of this variable (P<0/001) (Table 2).
Table 2. Comparison of the three groups (olive oil and sweet almond oil massage and control) with the time step criterion using repeated measures test

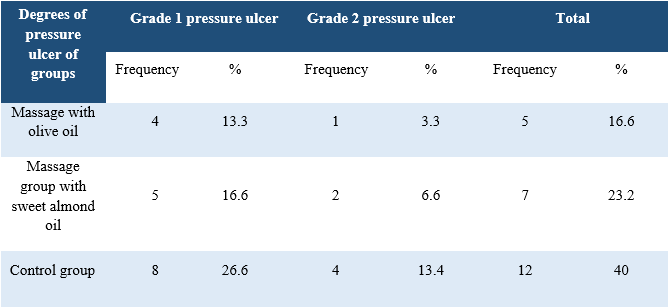
The results also showed that after the intervention 16.6% (5 cases) of the massage group with olive oil, 23.2% (7 cases) of the massage group with sweet almond oil and 40% (12 cases) of the control group suffered from first and second degree pressure ulcers after the intervention (Table 3).
Table 3. Comparison of absolute and relative frequency of degree of pressure ulcers in studied units
Results showed that there was a significant difference between the three groups (P<0.001) during the 7 days of bed ulcer prophylaxis. The control group started on day 3. Studies have shown the preventive effect of olive oil massage and sweet almond oil massage on the incidence of pressure ulcer. According to the follow-up tests, the olive oil massage group was significantly different from the other groups and had a slower trend in reducing the incidence of pressure ulcers (P<0.001).
The present study showed that olive oil and sweet almond oil massage are effective in preventing pressure ulcers. The preventive effects of massage with olive oil were more effective than massage with sweet almond oil. The results of various studies also show that topical use of olive oil is effective in preventing pressure ulcer in patients [32,31]. The present study is consistent with these two studies.
Studies on the effects of olive oil and sweet almond oil have shown positive effects on topical application of these two oils to the skin. Razi Zakaria found edible olive oil useful for the treatment of headaches, joint pain, anal ulcers and intestinal edema. It has also been shown to be effective for topical application in skin softness and vitality, prevention of perspiration and premature aging, treatment of seborrhea and scabies [33]. In addition to the skin softening effects, olive oil can also be topically applied in the treatment of skin problems such as psoriasis [34]. Topical and daily use of this oil has also been reported to be effective in improving the skin problems of premature infants, which may reduce the risk of skin infection [35]. Sweet almond oil with 54% oil is a rich source of vitamin E (26 mg per 100 g), group B vitamins, amino acids, minerals and 26% carbohydrates which can be used as skin massage oils. [36].
This article is the result of a Master's thesis, funded by Tehran University of Medical Sciences, School of Nursing and Midwifery. We would like to thank all the patients admitted to the ICU ward of Imam Jafar Sadegh Hospital of Yazd University of Medical Sciences and the colleagues who helped us in this study. This study has IR.TUMS.FNM.REC.1396.2687 code of ethics and registration code at IRC 20170124032147N4.
The authors declared no conflict of interest.
Received: 2018/03/9 | Accepted: 2018/03/14 | Published: 2019/08/28
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Articles Copyright © The Author(s).
Owned by Hamadan University of Medical Sciences.
Published by UMSHA Press
Journal Tel: +9881 38380150
Publisher Tel: +988138381795
Website: http://nmj.umsha.ac.ir
Email: managingeditornmj gmail.com
gmail.com
